

More babies on way, fewer docs to deliver them

It wasn’t because Mrs. Gong had terrible morning sicknesses or weird pregnancy cravings, but because there wasn’t a single obstetrics and gynecology clinic or hospital equipped with a delivery room in Gwacheon, a city close to Seoul with a population of 72,000.
“Usually, pregnant women like to have an obstetrician deliver their child when the time comes. So my wife had to go see an obstetrician who is located all the way in Pyeongchon because the hospital has a delivery room,” said Gong. “I heard from my wife that most mothers-to-be living in Gwacheon who are relatively well off go to hospitals or clinics in Yangjae or Gangnam, while others go to the one in Pyeongchon. It takes about 40 minutes by public transportation.”
Gong says the distant location of the obstetrician affected him and especially his wife both financially and mentally.
When his wife’s due date was approaching, Gong says she suffered mentally as well.
“For women in their last months of pregnancy, they have to be careful because you never know when you’ll encounter an emergency situation. My wife was also very tensed up in those months. If she gets into that kind of situation, there’s no hospital close enough with a delivery room for us to run to. It’s very dangerous for those women and, of course, the baby to not receive immediate medical care in a time of emergency.”
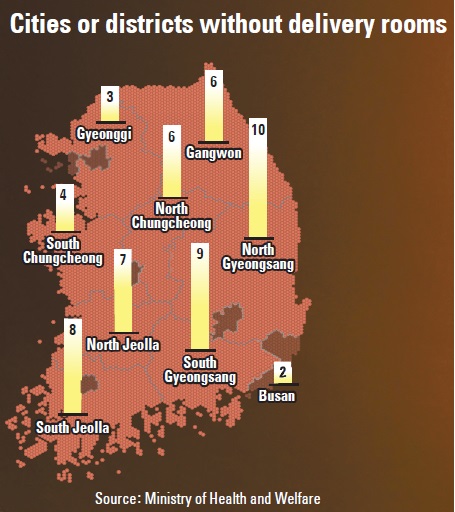
Gwacheon isn’t the only place without a hospital or an obstetrics and gynecology clinic equipped with delivery rooms. According to the Ministry of Health and Welfare, 55 cities and districts across Korea lack medical facilities where child delivery is possible. Patients must travel at least one hour by car to reach 48 of those locations. The ministry and the Health Insurance Review and Assessment Service designated those areas as “vulnerable areas for child delivery.”
Earlier this month, ruling Saenuri Party Representative Moon Jeong-lim said in a statement after the parliamentary inspections of the ministries that the number of medical facilities that are equipped with delivery rooms has tumbled by nearly half in nine years. Moon insisted that “there’s an urgent need to come up with countermeasures to save the country’s obstetrics and gynecology departments and improve Korea’s child-delivery environment.”
According to the statement, the number of medical facilities with delivery rooms dropped from 1,311 in 2004 to 739 in 2012 - a 44 percent decrease. The statement added that in the past five years, more obstetrics and gynecology clinics and hospitals have closed down than have opened.
Fertility rate inches up
Korea is known for having the lowest fertility rate among developed countries. The rate fell to an all-time low in 2005, at 1.08 children per woman, according to OECD statistics. Since then, the Korean government has tried repeatedly to increase that number, including providing financial support to women for each pregnancy. Thanks to these efforts, including the establishment of a presidential committee to tackle the “low birthrate in an aging society,” the fertility rate rose to 1.23 in 2010 and is predicted to rise again to 1.24 this year.
However, recent studies show Korea has the highest maternal mortality ratio among developed countries.
Until the early 1990s, many newborns in Korea couldn’t survive their first 100 days because of the country’s underdeveloped medical infrastructure for childbirth. Thanks to improved medical facilities, appliances and manpower, the infant mortality rate decreased dramatically. But now the country, which is known as one of the world’s leading health care providers, is facing a maternal mortality ratio that’s been increasing in recent years. Sadly, the country often called “medical Korea” is categorized as a less developed country when it comes to childbirth.
According to the World Health Organization, the maternal mortality ratio, is “the ratio of the number of maternal deaths per 100,000 live births from any cause related to or aggravated by pregnancy or its management.” Maternal death is defined as the death of a woman while pregnant or within 42 days of the termination of pregnancy.

Left: An obstetrician delivers a baby. The number of obstetricians and gynecologists has been decreasing in the country. Right: Newborns at an infant unit of a hospital. The country’s fertility rate has been steadily increasing. [JoongAng Ilbo]
The situation is even worse in rural areas such as Gangwon, which has the country’s highest maternal mortality ratio, at 32.1.
“The maternal mortality ratio in Gangwon is similar to the figures in Mongolia and Uzbekistan,” said Nah Seong-hoon, a professor of obstetrics and gynecology at Kangwon National University in Gangwon. “It’s for sure that the decreased accessibility to obstetrics risks the lives of pregnant women. It’s a shameful figure in such a leading country in medicine.”
On Feb. 3, a pregnant soldier who was serving at a military camp in Inje, Gangwon, died after failing to reach the nearest obstetrician. Lt. Lee Shin-ae, 28, was seven months pregnant and worked more than 50 hours a week at the front-line base camp in Inje. A day before her death, she started having abnormal symptoms, including vomiting. She fainted just after leaving her office. She was immediately taken to the nearest obstetrics hospital, a two-hour trip by car. The next day, she died of a brain hemorrhage after delivering the baby through a caesarean section.
After Lee’s death, the Korean government said it will take measures to improve working conditions for female soldiers, including locating obstetrics clinics or hospitals with delivery rooms in 48 areas that are designated as “vulnerable areas for child delivery.”
However, Nah said such a measure doesn’t go far enough.
“As you can tell from many statistical data, the number of obstetrics and gynecology clinics and hospitals are decreasing. The country is no longer producing as many professional obstetricians and gynecologists as before, and more and more existing hospitals and clinics in this field are closing down,” said Nah.
Park In-yang, secretary general of the Korean Society of Obstetrics and Gynecology (KSOG), who is also a professor at Catholic University’s St. Mary’s Hospital, agreed.
“The current measures taken by the government upon Lt. Lee’s incident is being pushed ahead without realizing the decreasing number of obstetricians and gynecologists in the country. Currently, there are not many obstetricians who can deliver babies in the country. But since all the newborns need to be delivered, the obstetricians have no choice but to force themselves to work more at nights and carry out emergency surgeries,” said Park. “This will definitely affect the maternity mortality rate. The government must come up with effective measures that can encourage the obstetricians and gynecologists in the country.”
Fewer residents entering field
According to the KSOG, the number of professional obstetricians and gynecologists has decreased drastically, with only 90 specialists entering the field last year, down from 253 in 2000. Among the 100 or so general hospitals across the country that train obstetricians and gynecologists, one-fourth are said to have no residents in those departments.
During a Sept. 29 National Assembly session concerning the collapsing medical supply system, Shin Jeong-ho, the former secretary general of the KSOG, said that “the department of obstetrics and gynecology is the department that resident doctors want to avoid the most.”
“Korea used to turn out around 300 professional obstetricians and gynecologists [per year] before, but the number dropped drastically to 90 last year. The department became unpopular among interns and residents to choose as their major. Such a phenomenon left professors of the department to engage in tasks that chief resident doctors do in general hospitals,” said Shin.
Shin added that the situation also affects the training of residents.
“Due to the lack of manpower in the department, the resident doctors in their third and fourth year who should be receiving training on delivering newborns, are engaging in tasks that first- and second-year resident doctors do, such as helping their professors,” said Shin. “Currently, more than half of the doctors who deliver babies are in their 50s. There’s a lack of young obstetricians who can deliver babies at the moment.”
A chief resident doctor surnamed Lee, 31, of the rehabilitation department at a first-level general hospital in Seoul, says he didn’t even consider applying for the obstetrics and gynecology department.
“The department of obstetrics and gynecology has long been considered the most unpopular department among interns and residents. The training itself is not that strenuous, but most of us think of the market at the time when we decided our major,” said Lee. “It’s a widely known fact that the pay is very low for obstetricians and gynecologists, however, the risk is too high. For those who open up their own hospitals or clinics, the maintenance expenditures are also very high.”
Lee said many hospitals with delivery rooms subscribe to private insurance as the doctors often face many lawsuits after medical accidents compared to other specialists.
“I heard the insurance fee for obstetrics and gynecology clinics and hospitals is a lot higher compared to other hospitals and clinics,” said Lee. “Then think about it, who would apply for such a department?”
Kim Sun-haeng, former president of the KSOG and an obstetrics and gynecology professor at the Korea University College of Medicine, said, “Until 2008, Korea was able to maintain a lower MMR than the OECD average because the obstetricians and gynecologists then worked with a full commitment of a doctor despite poor working conditions. However, it’s difficult to make young doctors bear the physical and mental burdens and sacrifice only with the ‘sense of duty of a doctor.’”
Won Dae-eun, 58, an obstetrician and gynecologist on Jeju Island, ran an obstetrics and gynecology hospital with delivery rooms from 1986 to 2009.
“To run an obstetrics and gynecology hospital with delivery rooms, it needs to be open 24/7 with a doctor who can deliver a baby as well as nurses who can help out. In most cases, there also needs to be an anesthetist on standby. But considering all the payroll costs, the medical fee for delivery is too low,” said Won, who is also the president of the Jeju branch of the Korean Association of Obstetricians and Gynecologists. “At first, when I started the hospital, I had about 200 deliveries per month. It was enough to pay for the maintenance expenses such as payrolls for nurses, the workers at the cafeteria, the laundry room and many more. But as time went by, the number went below 50 and I realized that it was difficult to keep the hospital that way. So I decided to close it down.”
Won renovated the building and operates a long-term care hospital there for elderly people, and a small obstetrics and gynecology clinic that no longer provides child delivery.
“Japan experienced the collapse of its child-delivery system many years back. I remember Japanese hospitals looking for Korean obstetricians with a Japanese license to work for them for a high salary. But that still couldn’t solve the deficit of obstetricians in Japan,” said Won. “So the Japanese government began establishing public delivery rooms across the country and hired midwives. For deliveries that are not so difficult, they made the midwives deliver the babies, while difficult ones were transferred to doctors. They also provided scholarships to resident doctors who signed a contract to become obstetricians when they finish training. But the Korean government has been standing idly on this issue for a long time.”
?In response to the recent phenomenon, the Korean Ministry of Health and Welfare said it has been providing financial support for obstetricians and gynecologists who can deliver babies in those “vulnerable areas for child delivery,” however, it sees the decreasing number of obstetricians and gynecologists as a “social phenomenon.”
“This year, we have completed providing a total of 1.25 billion won [$1.17 million] per medical facility, in which 50 percent of the cost comes from government expenditures while the other half comes from the local government in the area, to nine medical facilities,” a ministry official said. “With the financial support to existing medical facilities in that area, the owners hire obstetricians and install obstetrics and gynecology department with delivery rooms in the hospitals.”
Won said resident doctors at the obstetrics and gynecology department of general hospitals fail to receive sufficient training of delivering newborns, insisting that encouraging resident doctors to become obstetricians and gynecologists will not help increase the number of doctors who can deliver newborns.
“Many pregnant women prefer giving birth at hospitals with great service and experience, such as those operated by six or seven obstetricians, rather than general hospitals. Therefore, the number of deliveries decreases in such hospitals where resident doctors can train and experience delivering newborns,” said Won. “Moreover, the obstetricians at general hospitals don’t really give opportunities for resident doctors to have a go at delivering newborns because it’s so risky and they want to avoid getting into medical disputes. The government must come up with measures after deep considerations and studies.”
BY YIM SEUNG-HYE [sharon@joongang.co.kr]








with the Korea JoongAng Daily
To write comments, please log in to one of the accounts.
Standards Board Policy (0/250자)